|
Posted at AMPLE
26th July 2003 |
Questioning Market Leaders For Long Term Investors
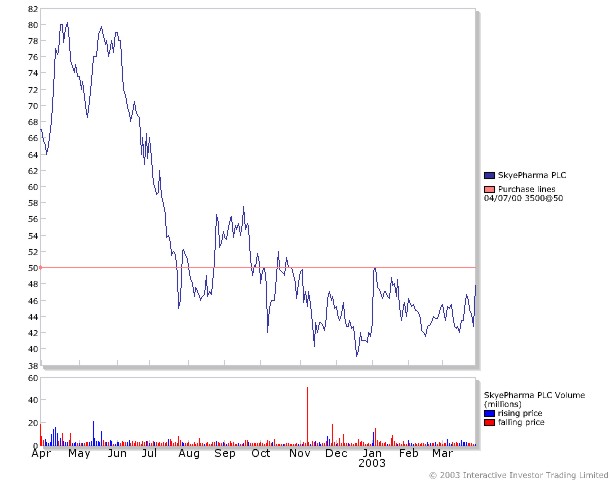
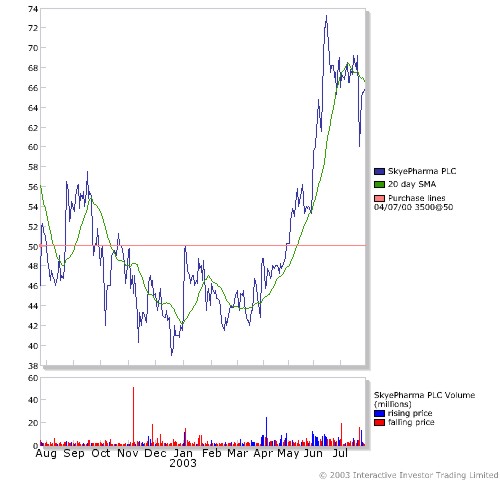
MICHAEL ASHTON - SKYEPHARMA PLC (SKYE)
CEO Interview - published 05/27/2003 |
|
Sector: drug delivery |
MICHAEL R. D. ASHTON is the Chief Executive Officer of SkyePharma
Plc. He joined the group in May 1997. His career of 31 years has been
totally dedicated to the pharmaceutical industry. Mr. Ashton's
experience ranges from working with Merck Sharp & Dohme in
Australia and in the US with Merck International and with Pfizer Inc,
where he held a number of senior management positions in New York and
internationally. Prior to joining SkyePharma, he was with Faulding,
Australia's largest pharmaceutical company, located in the US. As
Chairman and Chief Executive Officer of that company, he was
responsible for building the company to become well respected in the
industry, on NASDAQ and importantly profitable. With a Bachelor of
Pharmacy and MBA Degrees, he brings to the group a significant amount
of pharmaceutical experience, with a career in big pharmaceutical
companies and by having successfully grown value in smaller companies
by building them into fully integrated pharmaceutical organizations. |
|
TWST: Can we start out with a quick overview of SkyePharma? |
Overview |
|
Mr. Ashton: SkyePharma is a UK-domiciled drug delivery company. We
are some 20 years old. We have our origins in Basel, Switzerland. In
1996, the company, which was then a privately held company called
JAGO, did a UK IPO to form what is currently known as SkyePharma. We
have had an ADR listing in the US since 1998 so since 1996 we have
had the ability to access international capital markets. In going
over our business plan to move forward, our first objective was to
broaden the base of our drug delivery business technologies. At that
time we were a dominant player in the delivery of oral medication
through our drug delivery technology called GeoMatrix. We were also
an early entrant into the delivery of products for asthma using
breath- actuated inhalers and non-CFC aerosol inhalers using HFA
propellants. But I thought we needed a broader base, so we set about
expanding our portfolio of drug delivery technologies, both
organically through our internal processes as well as externally by
acquisitions. Today we believe that we are the largest drug delivery
company with respect to the number of drug delivery capabilities. We
have the ability to deliver products orally. We have now a leading
position in terms of delivering inhaled products for asthma, both
through dry powder inhaler (single and multi-dose) and non-CFC HFA
propellant aerosol technologies. In the sustained-release injectable
arena, we occupy a very large space: that's both via a dry-powder
capsule technology called BioSphere and a multi-vesicular lipid
matrix system which we call DepoFoam. These provide the ability to
introduce products into the body on a sustained-release basis, where
you may have an injection perhaps once every two weeks or once every
month rather than two or three times a week, thereby reducing the
number of unpleasant needle-sticks. We are also strong in the topical
arena (delivery through the skin), where we already have one product
currently on the market called Solaraze for actinic keratosis. So
with that span we cover about 90% of the drug delivery route
requirements that any biopharmaceutical company would require to
deliver any of their products. |
|
TWST: Does that make you the broadest-based supplier? |
Broadest Based
Supplier? Yes |
|
Mr. Ashton: Yes, it really does. There are others that are
approaching that. We were the first to actually identify that this
was the right way to go. There was a thesis some years ago that the
preference would be to be a dominant player in just one technology.
However the way I've formulated this company is that we are now
actually dominant in five areas, to the extent that we have centers
for excellence in five delivery technologies. The fifth one that I
didn't spend much time on was our solubilization technology which we
do use to improve the bioavailability of compounds for other
companies, but we largely now use this as an enabling technology to
expand the breadth of application of our oral, pulmonary and
injectable technologies in particular. |
|
TWST: What is the outlook for this market space? |
Market Space Outlook? |
|
Mr. Ashton: I think the outlook for the drug delivery market space is
excellent. The consensus estimates are that it will grow to $70
billion or $80 billion by 2007. I think there's no doubt that the
pharmaceutical companies, as they strive to build their product
pipelines, are now increasingly incorporating at an earlier stage
some drug delivery component to their promising compounds. However,
where we see our significant growth coming from is where we have been
able to identify unmet medical needs. |
|
To address these, we take a product that may be currently on the
market or a product that's come off patent, and develop an improved
version. We will then file a new drug application for either a new
indication or just a more distinctive indication. I'll give you an
example. We are close to filing a new product called DepoMorphine.
This is a sustained-release version of morphine, given as an epidural
(spinal) injection, that will provide post-operative pain relief
throughout the first 48 hours following an operation - the period of
peak pain. We believe it has the ability to completely replace
current pain control therapy, which is either given epidurally or
intravenously but on demand, when the patient is already in pain.
Patients today after operations do get pain medication with opiate
analgesics but that comes intermittently and only when their pain is
starting to get unbearable, so you have an uncomfortable patient.
DepoMorphine will provide a constant level of morphine in the body
and so give a steady state of relief of pain over that first 48 hours
which is really the critical time frame that you need to keep a
patient free of pain - and is also the time typically when you cannot
give a patient anything orally. We believe DepoMorphine is going to
be an important addition in this market segment. Morphine is a very
old drug. We've been putting up with suboptimal intravenous or
epidural injections or infusions of opiates for years. The
DepoMorphine approach is clearly a far better way to deliver
products. We've got various examples of compounds that we have taken
through to approval. Solaraze is a novel treatment for actinic
keratosis, a market that we believe is very under- diagnosed and
under-treated. It's a common condition and if left untreated a
certain percentage of patients will progress to a form of cancer
called squamous cell carcinoma. Actinic keratosis is a condition that
typically becomes evident around in your 40s and it arises from
having been sunburned at some stage in your life. Patients get these
little non-cancerous growths and although they are not painful they
do need to be treated as they have the same histology as skin cancer.
The problem is you don't know which one is going to turn into skin
cancer. So the best thing is to treat all AK lesions. We have
developed a simple gel that is simple to rub on. This will provide
the opportunity, we believe, to expand the usage base from the
dermatologist into the hands of the general practitioner, who is
usually the first line of diagnosis of AK but currently has to pass
patients on to the dermatologist for treatment. So we're using drug
delivery to create better value products, both for ourselves and for
pharma companies and biotech companies. Often the compounds that they
develop, in their initial form, are either impossible to dissolve or
not as commercially attractive as they would like. |
|
TWST: When you look at this space with that strong growth potential,
why isn't there more competition? |
Competition? |
|
Mr. Ashton: There is a lot of competition. In the oral area, most
pharma companies have some ability to try to look at different forms
of oral delivery and largely they can develop zero order delivery,
which is simply taking a product that, say, must be given 3 times a
day and reconstructing it so it will give an even absorption over
time in a once-a-day tablet. Where the difference comes is the
ability to have unique delivery systems. For example, some products
work better if held in the stomach for some time, and we have a
patented delivery technology which we call Parachute which simply
means it holds the product in the stomach and allows the product to
be absorbed through the gut wall. Conversely, it may be better to
deliver some products into a very specific site in the intestine,
which is a very good area in the digestive tract for delivery
directly to the liver. Again, some companies can have a product and
just simply coat it with an acid-resistant coating: this means it
will pass through the stomach but when it comes to the intestine,
which is alkaline, the coating is eroded and then the product
dissolves. We can do that with our technology but we can also go one
step further by designing the product whereby it will deliver in a
fairly narrow window in the intestine. A good example of that is
where we've improved the antidepressant Paxil for GlaxoSmithKline.
This is their largest product, with US sales alone of $2 billion last
year. This improved version is now on the market in the United States
where it is called Paxil CR. With Paxil CR, you take the tablet and
it moves intact through the digestive system and only starts to
release the active ingredient in the lower part of the intestine,
about five hours after swallowing the tablet. As clearly shown in the
clinical studies that they have carried out, Paxil CR causes
significantly less nausea than the original version of Paxil. A
well-recognized drawback of all antidepressant medications is a high
dropout due to nausea in the first few days of taking the product.
This is compounded by the fact that the antidepressant effect, relief
of symptoms, takes some weeks to be felt. Poor patient compliance '
patients who stop taking their medication ' represents a significant
cost to the healthcare system. By delivering Paxil CR through the
lower intestine, we have a product that not only produces less
nausea, particularly in the first week, but also has a greater
symptomatic relief in the early days. As early as the first week, the
patient is starting to feel some anti-depressive impact coming along.
So simply, here drug delivery technology has provided a better
product by delivering the active ingredient in a different format.
You're going to see more of these where we have the ability to create
a better product. Coming back to your question, there's a lot of
intellectual property out there that we have and other companies do.
There is competition out there certainly, but it's just not as broad
across as many spheres as SkyePharma has. |
|
TWST: What should investors expect from SkyePharma over the next two
or three years? |
What to expect? |
|
Mr. Ashton: We turned profitable in 2002, in line with a prediction
that we gave in 2001. We now have four key products currently on the
market, Paxil CR being one of them. Paxil CR could be a billion
dollar product from which we will get a royalty stream that would get
us in the range of $30 million in terms of free cash flow. We have
another product called DepoCyt, which is a cancer product. This is on
the US market and will be launched during the latter part of this
year in Europe; and we get a 35% return on sales. It's a niche
product that may ultimately get to sales of $100 million, but with a
35% return, you're getting a very attractive payback. We developed a
once- daily version of a product called Xatral for Sanofi-Synthelabo.
This is a treatment for the urinary difficulties associated with
benign prostatic hypertrophy, a common condition affecting
middle-aged males, and has been on the market in Europe since 2000,
with a US launch expected later this year. We get a mid-single digit
royalty on Xatral. For Solaraze, the topical gel for actinic
keratosis, we get a mid-teens royalty stream. Coming behind these are
two very important products. These were part of a deal we did at the
end of 2002 with Endo Pharmaceutical. We licensed them two of our
products, DepoMorphine, the pain relief product that I talked about
earlier, and the other product is called Propofol IDD-D, which is
aimed at the market for long-term post-operative sedation. The
biggest problem with the current propofol sedation products on the
market is that they are lipid- based emulsions. They attract
microbial contamination, just as milk would do if you left the bottle
open, and that means that after a few hours you have to throw away
all opened bottles and infusion lines that may be contaminated. We
have reformulated this product whereby it cannot support microbial
growth, so therefore we can use our version on a continuous basis. So
with our version you can put the patient in the intensive care unit,
with all the various infusion lines, and then put the sedative vial
in place. And when it's finished, you can just take the vial out and
put another one in. Our formulation of this product also decreases
the volume of fluid you're delivering into the patient |
|
Now here is a patient post-operatively who is in a supine position so
you really don't want to give them too much fluid as they are lying
down in the recovery phase, and you certainly don't want to give them
too much lipid. By putting these two critical care products together
in one transaction, we were able to license this group of products to
Endo for a potential of $120 million in milestone payments (with $25
million upfront) and with a potential to share up to 50/50 with Endo
in the profits at certain sale points. Importantly we have got new
products coming through to add to the products already on the market.
Each of these products has the ability, over the course of the next
three to six years, to generate about $30 million to $40 million a
year in terms of annual royalty for us. When you come down to the
collaboration we have with Endo for DepoMorphine and Propofol IDD-D,
that could generate, at the peak level of sales, revenues for us of
$100 million to $200 million a year. So we've got a lot of current
products on the market with substantial revenue and royalty stream
returns, and we've got a series of potentially major products right
behind that. And then we've got a very well supplied stack of
pipeline products behind that. So investors can see profitability
that's now happened ' and there are only a few companies in our space
that have been able to achieve that goal. |
|
However the key is sustained and growing profitability in the future.
We have given guidance for 2003 of œ100 million in revenues, so
let's say in round terms, $160 million US, with a significant
increase in profits, as obviously contributions leverage down from
revenue growth. Revenue growth is still largely driven by milestones
and so is lumpy but we've already got about œ100 million worth
of milestones from deals we've already constructed or are in place
that will be realized over the course of the next three years. So you
add those, plus the royalty streams, plus other new internal products
and deals that we've got in place with Pharma companies that we
anticipate landing and we believe you're going to see a very
significant increase in rising profits from SkyePharma over the next
few years. |
|
TWST: Do you have the team in place to support that? |
Support Team? |
|
Mr. Ashton: We do. We've got about 450 people worldwide, and more
than half of those are scientists. The bulk of the next level I guess
falls into the manufacturing. We have two FDA- and EMA- approved
manufacturing plants in Lyon, in the southern part of France, and in
San Diego, which are center for excellence for manufacturing our
products for Pharma companies. We have a very good clinical
regulatory group that can take products all the way through approval
in both the US and Europe and, importantly, we have a business
development group, which I think is second to none, with offices in
the US, Europe and now in Japan. We have people on the ground now in
Japan, a market that is important to grow. As you know, Japan is the
second largest pharmaceutical market in the world. So we've got a
very good management team to take the company forward. My own
background is largely in big pharma at Merck and Pfizer. I've run
public companies in the States and we've got seasoned managers, again
mainly from big pharma companies, but who know how to motivate people
in smaller growing companies. |
|
TWST: Do you have the financial resources you need? |
Financial Resources? |
|
Mr. Ashton: Yes. We are currently well cashed. We ended the year with
a little over $75 million in cash, which is sufficient to cover our
business plan. Our balance sheet will look like we're cash neutral in
2003 and that's largely only because royalties are usually booked as
accounts receivable, as they're normally paid a quarter in arrears.
If we brought both forward into 2003, then we would be certainly cash
generative. And we have been cash neutral for the last 18 months, so
we've been able to grow the business without needing new equity
finance. We've been able to increase our R&D spend in 2002 by 63%
over 2001 to about œ30 million thereabouts or $45 million and
we'll increase that up to about $53-$54 million this year. So it's
quite containable in terms of delivering what we need to do for our
plan with the cash we have. |
|
TWST: Is the market giving your credit for the progress you've made? |
Is Market
giving credit? No |
|
Mr. Ashton: That's always a good question. I don't think so, no. This
is a mixed up stockmarket, of course, we're in at the moment. I think
there was recognition certainly that we achieved our goal to be
profitable. I'm not sure that the full value of the creation of some
of the deals that we've put in place has yet been recognized. And
we'll see more deals going forward. The news flow from SkyePharma
will be very active. The deal on DepoMorphine and Propofol IDD-D that
I touched on with Endo is only for North America. We've still got
marketing opportunities or licensing opportunities in Europe and
Japan, which will be forthcoming this year and we've got a series of
other projects coming through. But no, I don't think the full value
of where we are is fully appreciated. The best rating is, of course,
when people see runs on the board in terms of looking at physical
sales, which now they can look at and we can report on. And as
investors get to understand that and get to understand the underlying
growth potential of the products that have our technology inside, I
think they will come to understand the valuation. We believe
SkyePharma currently is very under-rated. |
|
TWST: When you sit down with investors, what's the key message you're
trying to get across to them? |
Key Message? |
|
Mr. Ashton: I think it's largely that we have transcended from a
service-based drug delivery company, where the model was low risk but
low return. You did work for drug companies, they paid for it, but
because they paid for it, they gave you a fairly small return at the
back. Today we are aggressively identifying products in the
portfolios of pharma or biotech companies, going to them, putting
together some sort of transaction to work with their products. This
achieves a much greater value to us and we don't mind putting more
effort ' and investment ' behind that, particularly now we've got
clinical and regulatory groups in place to support the development of
products. The real creation of value for us is by taking products
further out in development ' taking a little more risk to the extent
that we are spending money on that. However remember that we are not
taking a great deal of risk on these products in as much as the
products we deal with are ones that have either currently been on the
market at some stage or at least have gone through Phase II so the
risk of clinical failure is low compared with that for a new chemical
entity. Taking products further on in development before out-
licensing gives us deal terms with fairly large milestones and
enjoying what I believe we deserve, which is a greater share of the
back-end profits. So the story we're telling of the value- added
creation of products is what we're about. We want to move away from
our roots as a contract drug delivery service provider, but to
continue to use drug delivery, if you will, as the R&D engine to
support the development of improved products which we'll license out.
The space we play in is that area from a time a drug leaves drug
discovery all the way through to manufacturing. Currently we do not
market products ourselves ' and frankly if we can put deals together
which can generate 50% share of the potential earnings of the
product, that's a very valuable model to have without having to worry
about a new skill set or the costs involved in setting up field
forces. Not to say that we may not look at that in the future in some
form, but currently I think our business model is very strong and
we'll be able to deliver the numbers at least that we have internally
signed on for. |
|
TWST: How are you going about trying to get that message out? |
How are you
getting the message out? |
|
Mr. Ashton: We are involved in meetings such as the one this
publication is for. We are represented at many of these conferences
and, of course, there is a very active investor relations process
through Europe and the United States. We have a head of investor
relations based in the United Kingdom and two people in the US
supporting that process. So we're very active in front of
institutions and potential investors.
TWST: Thank you. (TJM) |